CHUB: Consolidated Health Utilities
Project Context
The management of longitudinal medical records presents a significant challenge in the current healthcare ecosystem. Patients with chronic conditions often struggle to maintain, organize, and retrieve years of diagnostic history.
Although initial informal validation was conducted, a formal, rigorous understanding of the problem space was crucial for success. We embarked on an extensive research phase to map the ecosystem of both patients and healthcare providers.
Phase 1: Quantitative Surveys
We initiated the research with a broad survey to identify general pain points in the post-consultation experience. Synthesizing 80 responses, we focused on three core thematic inquiries:
- Theme 01What specific friction points do patients encounter immediately after a doctor's visit?
- Theme 02What methodologies are currently employed to manage and archive hospital reports?
- Theme 03Are there latent, pressing issues in the healthcare journey that remain unaddressed?

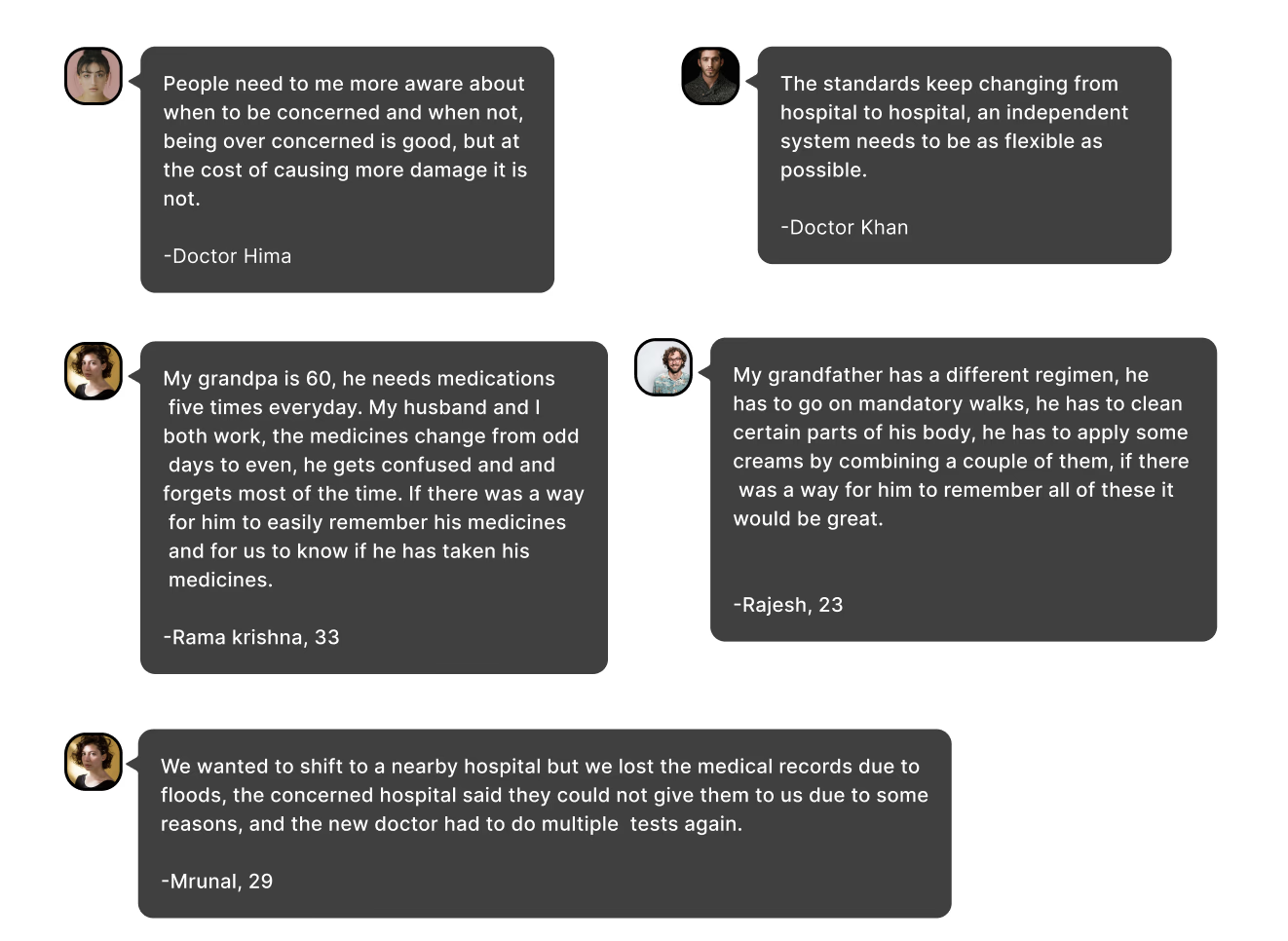
Phase 2: Qualitative Interviews
Building upon the survey insights, we conducted in-depth interviews with 2 doctors and 7 patients(including 3 with chronic conditions). The questions were contextualized for each stakeholder group.
For Doctors
- Current practices for handling longitudinal medical records.
- Major concerns regarding patients with chronic diseases.
- Expectations and requirements for a digital record system.
For Patients
- Workflows for handling and storing physical records.
- Pain points in retrieving historical health data.
- Post-consultation challenges beyond record keeping.
Synthesis & Definition
After days of brainstorming and analysis, we synthesized the raw data into actionable insights. This process culminated in a set of "How Might We" (HMW) statements that guided our design phase, transforming abstract problems into solvable design challenges.

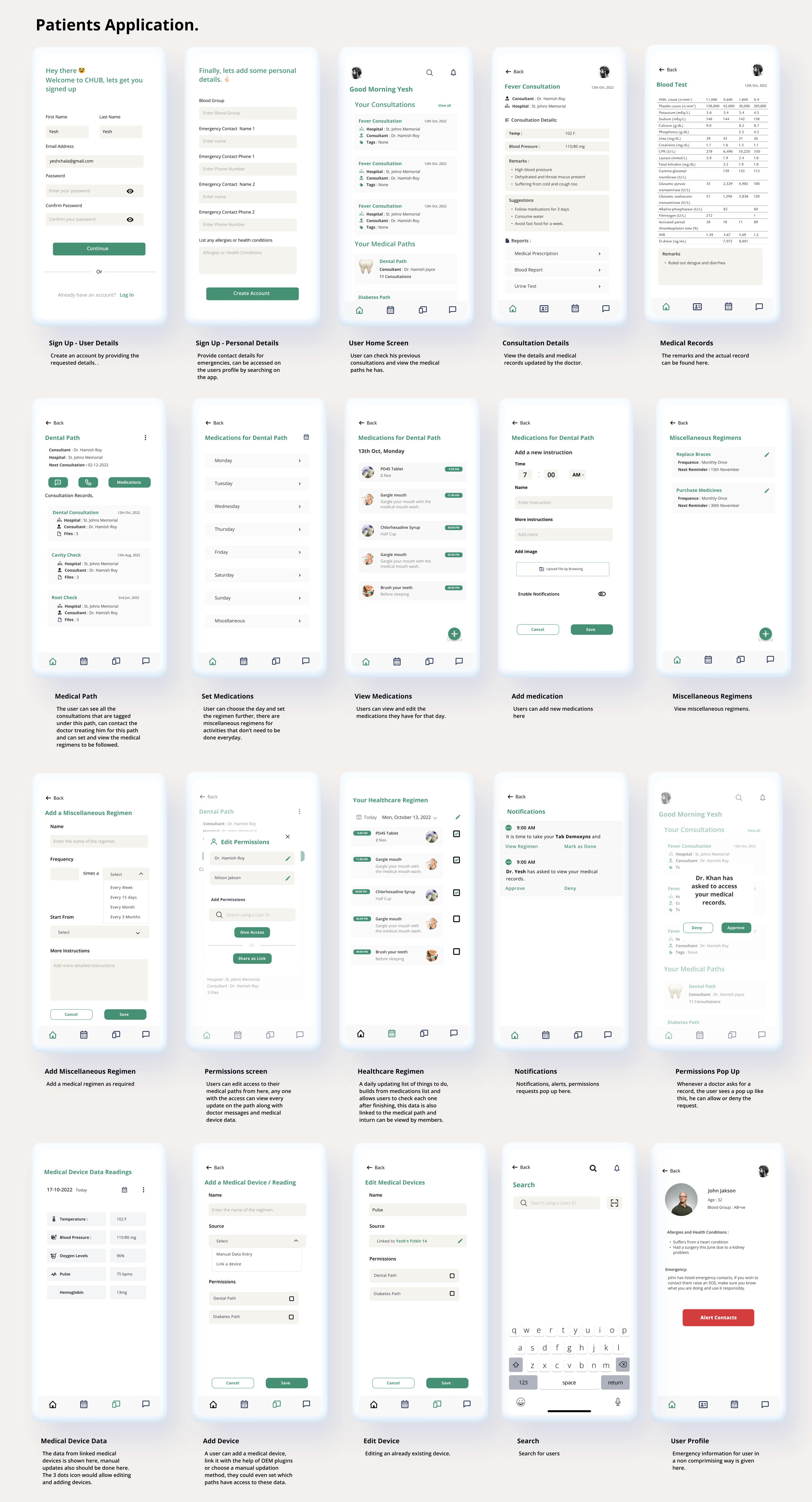
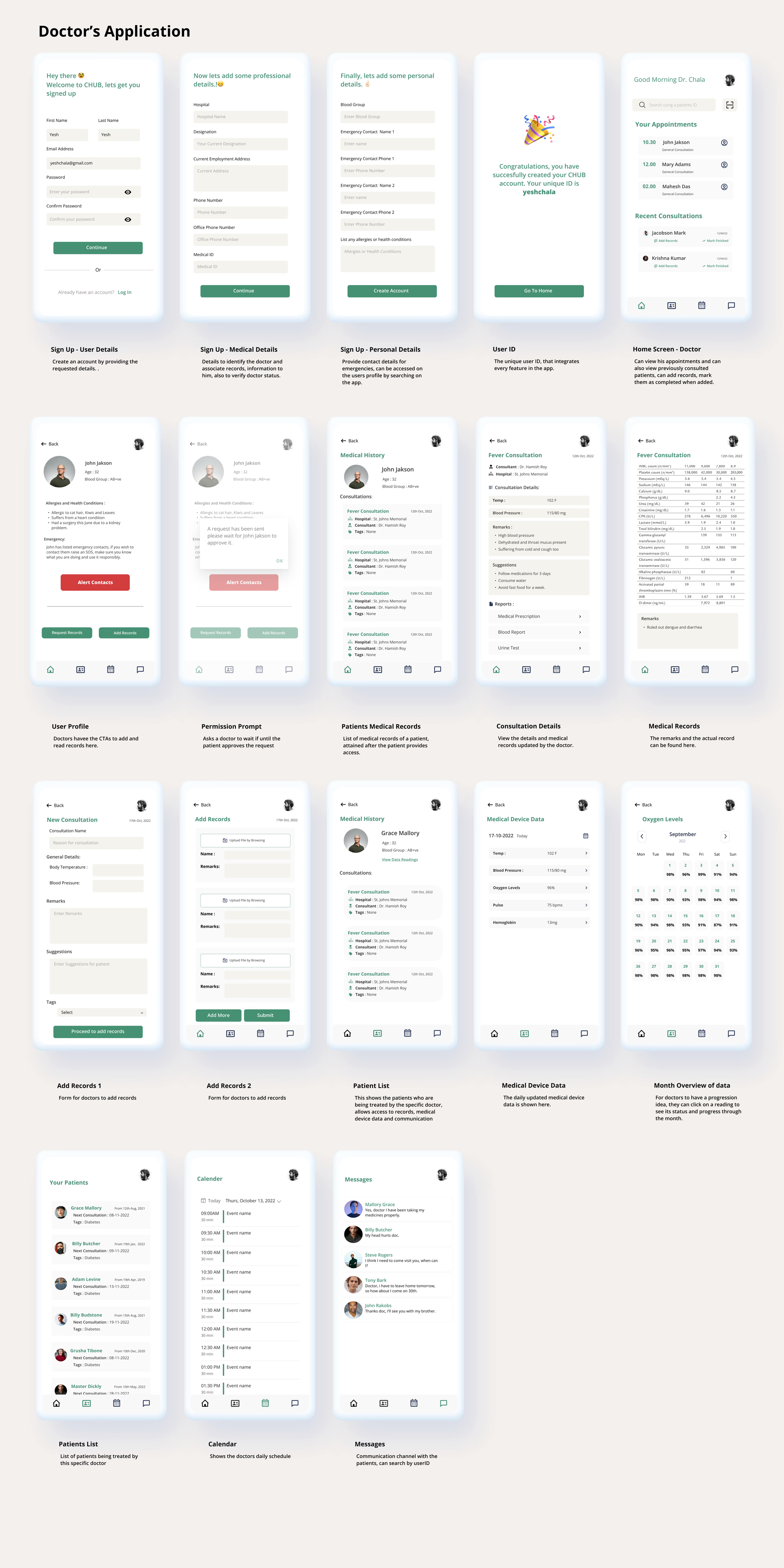
Designing the Solution
The Dual-App Strategy
Our research made one thing clear: Doctors and Patients operate in different realities.Doctors need speed, efficiency, and clinical precision. Patients need clarity, reassurance, and ease of access.
Consequently, we decided to design two distinct applications, each tailored to the specific mental model of its user base, rather than a "one-size-fits-all" compromise.

Evolution: From Paper to Pixel
The interviews and conversations over a 4-month period shaped our Information Architecture. We adopted a bottom-up approach, starting with low-fidelity sketches to validate our core flows.

Paper Sketches & IA
With initial clarity, we defined user flows and moved to Information Architecture. Finishing paper sketches was a pivotal moment—it offered the structural clarity we were missing and aligned the team on the system's logic.

6 Iterations to Final
Based on the sketches, we designed Version 1 prototypes. After the first round of testing, we refined, re-tested, and iterated. 6 iterations later, we arrived at the final solution that balanced clinical utility with user-centric design.
The Final Solution